Recently, they had a case of SIADH which I recognized easily and could get a reasonable differential diagnosis. The case included treatment with saline and desmopressin together. I thought a rare lapse in editing, expecting tolvaptan, but later it appeared again. So I looked it up. Apparently the vaptans have gotten too expensive. Since saline of the right concentration and right amount will correct hyponatremia, the barrier has been the safety of overcorrecting. Apparently desmopressin, while counterintuitive when ADH is already excessive, provides the protection against too rapid a rise in sodium with adverse neurological demyelination. Good to know my curiosity and inclination to challenge what seems suspicious has not been seriously impaired by retirement.
Showing posts with label NEJM. Show all posts
Showing posts with label NEJM. Show all posts
Wednesday, May 20, 2020
New Trick for the Old Dog
My subscription to the NEJM remains in force and I schedule two articles a week, even into retirement. Often the Case of the Week attracts me the most since it challenges my skills. I can usually get the differential reasonably close but some of the lab testing has passed me by, even in my own specialty where I recently fumbled with a presentation of Monogenic Diabetes. I knew the forms and the genetic identification but did not know how to correlate phenotype genetic results. More importantly, I did not know that the tests come as a commercial panel and that it is cost effective to order it, something that I avoided doing in my Medicaid and uninsured population, asking those patients to have their affected child tested for financial reasons.
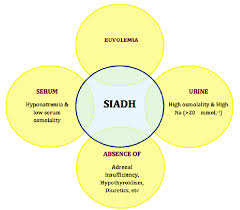
Recently, they had a case of SIADH which I recognized easily and could get a reasonable differential diagnosis. The case included treatment with saline and desmopressin together. I thought a rare lapse in editing, expecting tolvaptan, but later it appeared again. So I looked it up. Apparently the vaptans have gotten too expensive. Since saline of the right concentration and right amount will correct hyponatremia, the barrier has been the safety of overcorrecting. Apparently desmopressin, while counterintuitive when ADH is already excessive, provides the protection against too rapid a rise in sodium with adverse neurological demyelination. Good to know my curiosity and inclination to challenge what seems suspicious has not been seriously impaired by retirement.
Recently, they had a case of SIADH which I recognized easily and could get a reasonable differential diagnosis. The case included treatment with saline and desmopressin together. I thought a rare lapse in editing, expecting tolvaptan, but later it appeared again. So I looked it up. Apparently the vaptans have gotten too expensive. Since saline of the right concentration and right amount will correct hyponatremia, the barrier has been the safety of overcorrecting. Apparently desmopressin, while counterintuitive when ADH is already excessive, provides the protection against too rapid a rise in sodium with adverse neurological demyelination. Good to know my curiosity and inclination to challenge what seems suspicious has not been seriously impaired by retirement.
Friday, March 2, 2018
Keeping Engaged
As I experience some lumbar discomfort in what seems to be the left quadratus lumborum distribution, it is good to have very little running around and some desk time to study some medicine. There is some pretty good work floating around. NEJM has some articles on ICU experimentation with glucocorticoid + mineralocorticoid supplementation and different IV fluid options. I've been through the last six months of the Leonard Davis Institute Blog which has some items on how we practice. While the NEJM helps determine low value or high value interventions, we still do the things of low value. An LDI article looked at how docs would look at being penalized for doing things of limited value. They targeted use of urinary catheters to measure urine output in people not critically ill, use of cardiac monitoring without a preset end point, and use of ulcer prevention medicine in people who were not likely to get ulcers. I do not see too many catheters at my place. There are a lot of people on telemetry, mostly play it by ear. And proton pump inhibitors are now cheap and don't cause a lot of harm so people tend to get them irrespective of risk, though I've yet to see an ulcer develop during hospitalization, maybe because these were used or maybe in spite of them being used. So they asked if the docs who do these things should incur a financial penalty. Well, unneeded catheters can cause harm to people. Monitors cost somebody money. PPI's short term probably don't cause harm and don't cost much money though there seems to be some correlation of acid inhibition with opportunistic infections so maybe they do. Like the majority of the respondents, I have relatively little sympathy for the hospital or insurer making less money than they could have, which would be the outcome of less monitoring. Having insurance premiums go up because of these expensive days is a little more problematic so the societal cost does merit some consideration, as it did to those polled. And the catheters are a no-no as they harm patients.
However, we all do non-productive things. The residents order Mg and Phos on everybody and then give IV replacement for trivial variances. These people will have the same variances at home, undetected by the lab, and do just fine ignorant of those results and absent any intervention. We do ac and hs glucose monitoring and supplemental insulin on all diabetics. Probably nobody's microvasculature will be improved from this practice though for some people it does help recommending chronic insulin dosing. We are just not selective about this. We have acts of omission too. I've yet to see a resident include a rectal exam in the initial H&P, irrespective of its value. Reviews of old records leave a lot to be desired. These cost nothing, can add a lot of value, sometimes save money on not repeating things that will not have changed and infuse a habit of thoroughness that reaps its rewards later. We are just not selective enough or thoughtful enough in what we do.
But penalties for excessive care? Being punitive rarely improves care and probably wouldn't here either.
However, we all do non-productive things. The residents order Mg and Phos on everybody and then give IV replacement for trivial variances. These people will have the same variances at home, undetected by the lab, and do just fine ignorant of those results and absent any intervention. We do ac and hs glucose monitoring and supplemental insulin on all diabetics. Probably nobody's microvasculature will be improved from this practice though for some people it does help recommending chronic insulin dosing. We are just not selective about this. We have acts of omission too. I've yet to see a resident include a rectal exam in the initial H&P, irrespective of its value. Reviews of old records leave a lot to be desired. These cost nothing, can add a lot of value, sometimes save money on not repeating things that will not have changed and infuse a habit of thoroughness that reaps its rewards later. We are just not selective enough or thoughtful enough in what we do.
But penalties for excessive care? Being punitive rarely improves care and probably wouldn't here either.
Subscribe to:
Posts (Atom)